Scenarios are just great.
We’ve posted a number of scenarios here over the past couple years as part of our Live from Prospect St. series. These are usually nuanced cases requiring a critical diagnostic approach, and we love to dive deep and discuss all the nitty-gritty angles and considerations. It’s a nice way to learn.
There’s another benefit of scenarios, however, which I don’t think we’ve been able to achieve. The simple fact is that when you first graduate from EMT class and enter the field, there’s a great deal of stuff you need to learn. Not the textbook stuff, but the street stuff. How to manage the flow of a call, approach a scene, identify people with useful information. What kinds of diseases are common and their typical presentation (versus the uncommon, atypical stuff that textbooks love). How to monitor a radio, find an address on the map, and coordinate with other responding resources. Clinical judgment and how to apply it. That sort of thing.
It’s what you learn over time as you develop experience. And while one of the goals of a good education is to shorten that learning curve, there are some aspects you just can’t teach; you have to live it.
But scenarios can help. Because they resemble real life, they can help you understand what real life “looks like,” before you’ve spent enough years on the road that you’ve learned it the hard way. A handful of interesting scenarios isn’t enough; you need to see all the other stuff, the sheer volume of humping routine, typical patients through routine, typical situations.
So while we plan to continue the Live from Prospect St. series, we’re kicking off a new project as well: Scenarioville!
Scenarioville is an imaginary city in a parallel universe, and you work there — so to speak. Unlike our previous scenarios, this will be a consistent environment that you can learn your way around. There’s a fixed map with specific destination hospitals, an emergency system and resources you can get to know, and an equipment list that won’t change on you.
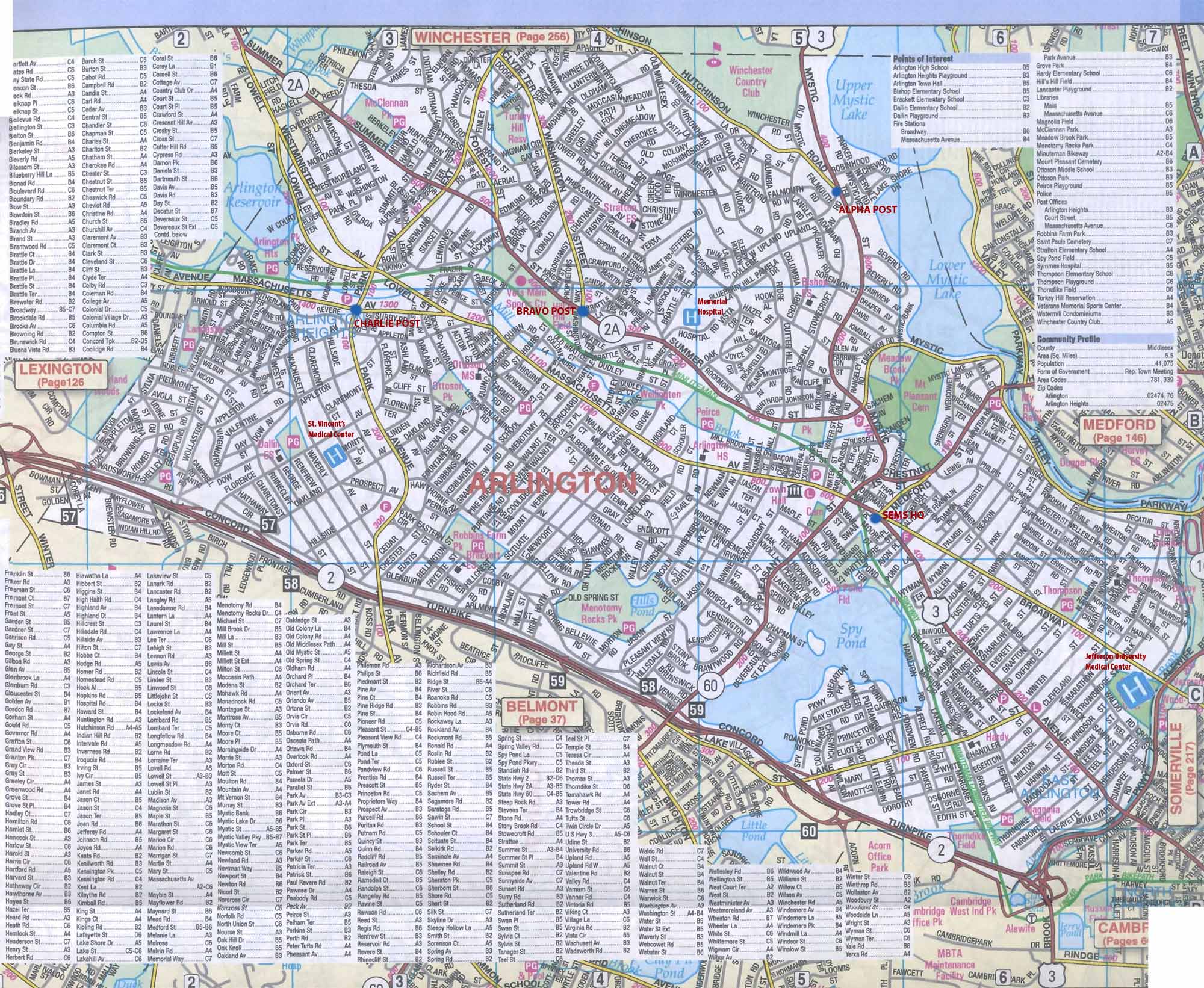{kind=link}
Just like in real life, this means you can “get the hang” of working in a real EMS system. You’ll be dispatched with an audio clip (a transcript is provided if you’re playing via smartphone or other device without audio capability, but if possible, try to use the recording for realism), locate the address in the “mapbook,” respond to the scene, make the decisions, and later learn the outcome. We’ll be posting at least one scenario per week — broken into segments as we usually do, but to minimize clutter, updates to each scenario will simply be added on to the existing story rather than posted as separate chapters.
These cases won’t all be interesting or emergent or in any way unusual; many will simply be standard EMS fare. They’re based on reality, but they’re fiction, and debriefing discussions will be short and to-the-point. Over time, as you play our little game and slog through call after call, you’ll hopefully start to develop something suspiciously like experience. It won’t be the same as really working out there… but it’ll be closer than the textbook.
Make no mistake, this is intended for new folks. The truly green EMT fresh out of class without any experience needs this type of drilling, and it’ll bring him much closer to functional competence prior to the day he puts on his first uniform. Experienced providers may find this suspiciously like, well, work, but they’re still encouraged to play along and lend a grizzled voice.
The first scenario is up now. Take a look, let us know what you think, bear with any initial rough edges, and stay tuned for more!
Recent Comments