See also what Agonal Respirations, Seizures, and Cardiac Arrest and CPR look like
Jugular vein distention or JVD (alternately JVP — jugular vein pressure or jugular vein pulsation) is right up there among the most mentioned but least described clinical phenomena in EMS. If you tried to count how many times it occurs in your textbook, you’d run out of fingers, but many of us graduate without ever seeing so much as a picture of it, never mind developing the acumen to reliably recognize it in an emergency.
JVD is simply the visible “bulging” of the external jugular veins on either side of the neck. These are large veins that drain blood from the head and return it directly to the heart. Since they’re located near the surface, they provide a reasonably good measure of systemic venous pressure.
JVD is elevated any time venous return is greater than the heart’s ability to pump the blood back out. Remember that we’re not talking about the vessels that plug into the left heart; that involves the pulmonary arteries and veins, which are not visible in the neck. (Instead, the best indicator of pulmonary hypertension is audible fluid in the lungs.) Rather, we’re talking about the systemic vasculature, which drains into the right ventricle via the right atrium. When veins aren’t getting emptied, we look downstream to discover what portion of the pump is failing. JVD is therefore caused by right heart failure. (Of course, the most common cause of right heart failure is left heart failure, so that doesn’t mean it’s an isolated event.) If JVD isn’t the heart’s fault, then we look to fluid levels. Too much circulating volume will lead to bulging veins for obvious reasons; the flexible tubes are simply extra full.
Although it’s probably most often seen, and most diagnostic, in volume-overloaded CHF patients, the main reason JVD is harped upon in EMS is because it’s a useful sign of several acute emergencies. Mainly, these are obstructive cardiac conditions, where some sort of pressure is impeding the heart’s ability to expand, and immediate care to relieve the pressure is needed in order to prevent incurable deadness. Much like the bladder, the heart is just a supple bag of squishy muscle, and although muscle is very good at squeezing, it has no ability to actively expand. The heart therefore fills only with whatever blood passively flows into it, and if it’s being externally squeezed by pressure in the chest, it can’t fill very much.
Tension pneumothorax is perhaps the most common cause, where air leaks from the lungs into the chest cavity with no way to escape; as the pressure in the chest increases, it bears down on the heart. Associated symptoms are respiratory difficulty, decreased breath sounds on the affected side, and hypotension. Pneumothorax can be readily corrected by paramedics using needle decompression.
Cardiac tamponade is another cause, where fluid leaks from the heart into the pericardium, an inflexible sac that surrounds it (this leakage is called a pericardial effusion), eventually filling the available space and compressing the myocardium. Associated symptoms are hypotension and muffled heart sounds (these plus JVD are known as Beck’s triad). Tamponade cannot be treated in the field, but an emergency department can perform a pericardiocentesis, where a needle is inserted through the pericardium. (For the medics out there, electrical alternans on the monitor is also supportive of tamponade.)
A rather less common syndrome that can produce similar obstructive effects is severe constrictive pericarditis, inflammation of the pericardium usually caused by infection.
JVD is not an all-or-nothing finding — the amount of distention visible at the neck will depend on the degree of venous pressure. Gravity wants to pull blood back down, so the more venous pressure, the higher on the neck distention will climb; profound JVD reaches many inches up the neck, slight JVD will only cover a few centimeters. The pressure can actually be quantified by measuring the vertical height of the highest point of distention (measured from the heart itself, using the angle of Louis as a landmark), but this is probably more detail than is needed in the field. Suffice to say that distention reaching more than 2-4cm of vertical distance (as opposed to the distance on the neck) above the chest is usually considered pathological, and less than 1-2cm can be considered suggestive of hypovolemia.
If it changes with respiration, JVD should rise during expiration and fall with inspiration. Breathing in involves using your diaphragm to create “suction” in the chest, reducing pressure and allowing greater venous return — draining the jugulars. A paradoxical rise in JVD during inspiration (think: up when the chest goes up) is known as Kussmaul’s sign (not to be confused with Kussmaul respirations, which is a pattern of breathing), and is particularly suggestive of obstructive pathologies.
JVD can be difficult to appreciate in all but the most significant cases. It helps to turn the patient’s head away and illuminate the area with angled backlighting, which creates a “shadow” effect. Jugular pulsation should not be confused with a visibly bounding carotid pulse. To distinguish them, remember that although jugular veins may visibly pulsate, their rhythm is generally complex, with multiple pulsations for each single heartbeat (you can feel the carotid to compare the two). The jugular “pulse” will also never be palpable; the distention can be easily occluded by the fingers and will feel like nothing.
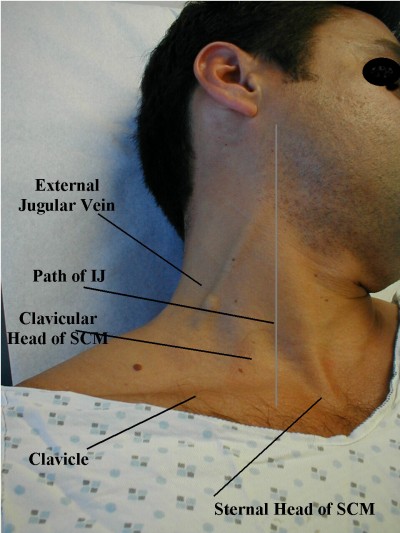
Strictly speaking, the internal jugular is usually considered more diagnostically useful than the external jugular, but it’s far harder to examine, so the latter is often used. For various reasons, many people also find the right jugular more useful than the left, although in an ambulance it’s harder to examine.
Most often, JVD is examined in an inclined or semi-Fowler’s position of 30-45 degrees. If the patient is supine, a total lack of visible JVD is actually pathological and indicative of low volume; in this position the jugular veins are usually well-filled. (Think: flat veins in a flat patient is bad.) JVD when the head is elevated is more to our interest.
Some examples of visible JVD follow, plus some examination tips. It is recommended that you start checking this on your healthy patients now, so you’ll know what it looks like before you try to make a diagnostic call using its presence. And until you do, stop documenting “no JVD” on your assessments!
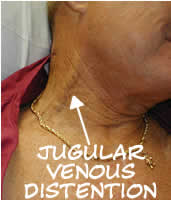
Significant JVD

A different, much larger view of the same (click to enlarge)
Click through for a good discussion of JVD assessment

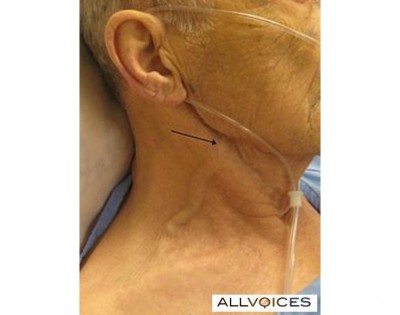
Some more subtle JVD
The basic method of measuring JVD
A nicely thick and squiggly external jugular
Here’s a student making her external jugular “pop” by heavily bearing down, aka the Valsalva maneuver. This markedly increases thoracic pressure, increasing venous backup; it’s an exaggeration of the effect seen during normal exhalation.
Another example of someone inducing JVD by a Valsalva
Here’s a great video demonstrating the appearance of JVD, how to measure it, and testing the abdominojugular reflex (formerly known as the hepatojugular), which involves pressing down on the abdomen to raise thoracic pressure.
A brief clip of jugular venous pulsation, visible mainly toward the suprasternal notch.
http://www.youtube.com/watch?v=sOpn6_r7Wo4
Good stuff.
Imagine the looks we will get walking into an emergency room: “He’s got a CVP around 20 or so.”
One eye-roll from the triage nurse won’t be enough; she might have to activate the whole team.
Field connection time!! I read this entry, thought about it, and went to work. I’d never actually seen JVD before, so it was interesting to me. Literally, that same day, we had a very badly hurt patient, and I am beyond thrilled to say that I looked at the patients neck and actually noted the JVD, thanks largely in part to this entry! The patient wound up going to a hospital with more capabilities for treatment, and some of that was due to that finding.
Thank you thank you thank you!!
No, thank you 🙂
Brandon,
Great site! It’s been awhile since I worked with you out of Echo and just wanted to say that you are helping fill an educational void with this material. I myself was “lucky” to see JVD, agonal breathing and different types of seizures in my first 6 months on the job where some can wait years to do so. Once you see them in person, you never forget. In the meantime, your articles are helping others “fill in the blanks”. Keep up the good work!
Mike,
Small world! Been a while indeed; great to hear from you again.
Very helpful on a topic that, yes, is WAY talked about but never really shown. I remember learning to check for JVD as a newbie EMTB in 1999 but didn’t know what it actually was for years. Good stuff!
I am 41, healthy, not over weight female and I’ve been experiencing this a lot lately. I don’t ever look at my neck to see if its moving but I sure can feel it. On both sides though, it comes and goes. Should it be something to worry about??
Michelle,
I’m afraid I can’t give out medical advice here — not that you’d want it. See your doctor!
Michelle, you could be experiencing a type of arrhythmia (most commonly an SVT, or premature beats). Go and get a check up, especially if it lasts for any length of time or you have other symptoms including dizziness.
Hi both sides of my neck have jvd, my right shoulder and arm has also swollen after first noticing 4 days ago. I’m also experiencing pain and discomfort. It will be 4 more days before I can get to a doctor. Should I be worried about a possible heart attack.
Isn’t there a difference between JVD and JVP?
The distance of pulsation and actual distension are often much much different. At times you cannot even see JVD, but you can still see the pulsation.
Are they really to be treated as the same thing?
Well, the actual pattern of the pulsations can be useful in some advanced diagnostics. But otherwise, the goal is to assess the height of the column of blood within the vein. If you can see the pulsatile meniscus at the top of that column, then you’ve done that. Sometimes the vein itself is prominent even without blood, depending on how well-developed the vessel is, and how thin or demonstrative the surrounding tissue may be; if unsure whether you’re seeing a fluid column or the vein itself, you can sometimes “strip” the vein to empty it and then let it fill from below. (Pin the vein from above with one finger to prevent filling from above, then use another finger to strip it downward. That will show the vein empty. When you release the bottom finger, blood will fill from below, revealing the JVD height.)
That being said, when you see a prominent neck vein it is typically the external jugular. Ideally you would use the INTERNAL jugular for this sort of thing, and you can usually only see the IJ from its pulsations anyway.
I have a hump that is much larger than the vein ( 1/3 of a tennis ball or so ) which swells out on the right side of my neck on & off . I find that it does this and is more pronounced when stressed or mad or maybe higher blood presure . There is no pulsation to speak of and no portruding vein as in photos above , so I am not sure what it could be . It seems that the skin inflates with liquid kind of like a giant blister ( but not a hard mass ) that goes away after a while …………any help would be great knowledge because doc has nothing !
Better off speaking with a medical provider in person than on the internet!
My son has internal jugular phlebectasia (aneurysm of the internal jugular vein) and the symptoms you describe occur on valsava maneuver or other intra thoracic pressure. (Laughing, a lot of talking or raising his voice, blowing up a balloon, etc.) Valsava maneuver is a good test. Ultrasound is diagnostic test. Alternative diagnosis could be laryngeocele.
I have that too… it appeared after JVD one night that I had for hours (and honestly I didn’t go to ER because of the experience I had there a few days prior). None of the doctors could tell me… if you ever figured it out… I’d like to know! ASAP!
Hi there I am so happy I found your site, I really found you by accident, while I was researching on Yahoo for something else, Anyhow I am here now and would just like to say
cheers for a incredible post and a all round thrilling blog (I also love the
theme/design), I don’t have time to read through it all at the minute but
I have saved it and also included your RSS feeds, so when I have time
I will be back to read much more, Please do keep up the
awesome work.
I’m 19 years old and my left jugular vein is noticeable at all times and hurts at some points whereas my right side is “normal”. I’m in my second year of nursing school and all this learning about heart failure is scaring me!
Hi I have like a swollen looking vein on the right front of my neck… No pain or discomfort..it goes the whole distance from top to bottom..my Dr said it’s nothing.. It’s very noticeable should I get a second opinion thanks
Irene, you don’t want an opinion from the internet!
“Immediate care to relieve the pressure is needed in order to prevent incurable deadness…” I love it! I have right-sided CCHF, and I have a visible jugular pulse on the right. I read this piece for info.When I got to that part, I laughed myself silly! Thank you for that — we all need a laugh once in a while, no matter how serious the subject. Right — we DO want to prevent incurable deadness if at all possible…
Thanks again!
Wow! Im a junior in Highschool and am in an EMR Class, about to run my assesment which determines if I get certified or not…. this is just getting me ready for anything my proctor throws at me!!!! Thanks
I can’t tell from the article, do things like laughing/bearing down/etc naturally cause JVD in healthy people? Or can you do those things to actually test for JVD?
They’ll transiently elevate the JVD. Evaluating the JVD as a diagnostic maneuver generally uses its level at rest, at end expiration.
I have have pulmonary stenosis and recently have noticed an enlargement of my right jugular vein. I have been to two different doctors and got two ultrasounds. Both said I was okay but couldn’t tell me what was happening, it just makes no sense. My blood work, O2 levels, and BP are all normal. I am an avid runner and for all intensive purposes am really healthy. What should I do?
My Auntie passed away a few days after seeing her last year. I saw her struggling due to sickness and diarea and her diabetes. She had been prescribed medication by her gp to help her get over the sickness and diarea over the phone. I remember seeing her neck vein prominently in her neck and pulsating. Although this alarmed me, I thought it was due to her bieng unwell and was kind of reassured by the doctor telephone call. However upon learning of her cause of death bieng CAD and diabetes I have been searching for something. I believe now if I had known what this JVD meant I would have been able to call 999 and she may still be here. Although I knew nothing of this at the time I’m happy to know this now as I may be able to help someone else in the future.
I had an ICD implanted two weeks ago. The day after implant I developed a DVT in the subclavicle vein. The swelling in my left arm quickly resolved after being given elequis. Now after two weeks I see that my left external jugular vein is distended. The right isn’t. Could this be a result of the clot? If not, is there another reason that the distention would be on only one side?
Thank you for the article. It is the best discussion of JVD that I have found.
I’m wondering how temporary this can be, and what a super brief episode might indicate.
This evening after a 5K, I felt a muscle spasm on the right side of my neck, and when I looked in the mirror an hour or so later, my right jugular vein was shockingly prominent. It gradually went back down to normal over the next few hours.
Background: I am a lifelong super-fit endurance athlete. Two to three years ago, I had an avalanche of health attacks–a hyperthermia injury, a tick-borne illness (received doxycycline), followed rapidly by probable gastric ulcers, and then covid and two months of long covid POTS. I had some arrhythmias that led to monitoring, but all my arrhythmias went away and I returned to long distance running. I still have stomach flare-ups (bloating) that feel like a constrictive chest pain, and in the worst cases I seem to have dramatic blood pressure fluctuations. I have been to the ER multiple times and always told my heart is super healthy; then they usually prescribe for acid reflux, except that I don’t actually experience much acid reflux anymore, just stomach bloating. (I had much more significant reflux when I was younger.) So, for the past week, I have had an especially bad flare up of the apparently gastric chest pain. But my circulation seems completely adequate, such that during today’s 5K, I did not have to breathe as hard as most other runners around me. And yet, afterwards, there it was–a purported telltale sign of right-side heart failure (i.e. my episode of JVD). I don’t know what to make of this.
Sorry, “two to three years ago” should be a little over 1 to a little over 2 years ago.
Hi John. Transient JVD can occur from just about anything that changes the pressure in the chest, such as bearing down. But you’d really have to discuss with your healthcare team; medicine is hard, but “comment section” medicine is harder!